Objective
The Dartmouth Health system Quality Committee supports building systems and removing barriers to deliver evidence-based care for all Dartmouth Health patients with opioid use disorder, including screening to identify patients and offering immediate access to medication treatment and counseling with longitudinal follow-up.
Background/Rationale
- Long-term treatment with one of three FDA-approved medications is the most effective approach to opioid use disorder (OUD). Opioid agonist treatment (OAT-buprenorphine and methadone) results in a 70% reduction in all-cause mortality compared with detox, and dramatic improvements in function/quality of life. Naltrexone monthly injection is another option for selected patients.
- In the US, only 10-20% of those in need of treatment for OUD receive it, and the care is often not evidence-based (70% of those in treatment do not get OAT) or longitudinal.
- Persons with OUD are commonly ambivalent about recovery. Prompt initiation of medication during “reachable moments” improves outcomes. Waitlists and other delays in treatment markedly increase the risk of death.
- Starting buprenorphine as an inpatient and linking the patient to care is more effective than detox and referral (72% vs. 12% engagement in ambulatory treatment), and is standard of care at other New England academic hospitals.
- Patients with OUD admitted to the hospital often engage in disruptive and unsafe behaviors, are non-adherent, and leave against medical advice. Treating withdrawal and craving with OAT improves patient comfort and cooperation, treatment outcomes and staff safety.
- Starting buprenorphine in the ED doubles engagement in ambulatory treatment compared with referral and outreach alone.
- Many (but not all) patients can be effectively treated in primary care, which reduces barriers to access and integrates OUD treatment with treatment of psychological and physical co-morbidities. However, survey data shows that the majority of DH PCPs are not confident in their ability to treat alcohol and substance use disorders, and are dissatisfied with the resources currently available. <20% of PCPs are waivered to prescribe buprenorphine and the majority of those have not prescribed yet. Half of the unwaivered clinicians are not interested. Waivered PCPs are unwilling to prescribe without in-clinic behavioral support available.
- OAT saves money: buprenorphine treatment reduces annual total health care costs by ~$20,000 per person through improving health and reducing ED and inpatient use.
- The “Moms in Recovery” program has been providing evidence based treatment for patients with OUD in the outpatient and inpatient (obstetrics) setting for over two years. The program was recently awarded a $2.7 million grant to spread their model throughout New England.
Additional background resources
Note: To access some of these resources you must be on the DHMC network.
- Sarah Wakeman’s DHMC Medical Ground Rounds 12/15/17
- Knowledge Map guideline: Primary Care Based Treatment of Opioid Use Disorder
- New York Time’s op-ed on the importance of medications in treating OUD
- Using Science to Battle Stigma: OAT saves lives
- Integrating Opioid Use Disorder Treatment into the Hospital Setting
Aspirational goals
- All clinicians and staff will recognize OUD as a treatable chronic disease that, like diabetes, needs to be addressed. Screening for and evidence-based treatment of OUD will occur in a non-judgmental, stigma-free environment. As with other chronic diseases, treatment is best done through a longitudinal multi-disciplinary approach with linkage to community resources.
- All inpatients with moderate-severe OUD will be identified through screening and encouraged (through education and motivational interviewing) to start on medication and counseling for OUD during their admission. Patients in acute opioid withdrawal will be promptly treated with OAT.
- Patients presenting to the emergency department with OUD will be identified through screening and offered medication and counseling.
- Patients started on buprenorphine (or methadone) maintenance will receive a “warm hand-off” to ongoing outpatient treatment, with a follow-up appointment <7 days from discharge. Patients started on naltrexone will receive Vivitrol injection before discharge.
- Multidisciplinary treatment of OUD will be “mainstreamed” into primary care as the Collaborative Care Model is rolled out in Dartmouth Hitchcock clinics. “Hub and spoke” relationships with specialty addiction treatment facilities will allow patients to receive the proper level of care and supervision.
Potential barriers
- Attitudes/Culture/Misunderstanding
- “Not my job” vs. “we should turn toward patients with OUD…”
- Addiction as willful misbehavior/moral failing vs. treatable chronic disease
- OAT as “replacing one addiction with another” vs. highly effective evidence-based standard of care
- Current policy/procedure/eDH create barriers instead of facilitating proper care
- Buprenorphine for Opioid Use Disorder in Adult Patients Policy and Buprenorphine Induction for Opioid Use Disorder in Adult Patients Procedure: “BIT team must be consulted and must agree that buprenorphine is indicated prior to inpatient induction.” Clinicians are not allowed to initiate buprenorphine to treat withdrawal or addiction until permission is granted.
- Buprenorphine Induction Order Set: BIT team must be contacted prior to initiating buprenorphine therapy.
- Buprenorphine Inpatient Order: requires positive urine for buprenorphine in past 2d, name and phone number of pharmacy, name and phone number of authorizing provider. These are unnecessary barriers to ordering, and are not met by a patient self-treating with “street” buprenorphine.
- Lack of adequate human resources to meet current needs
- Behavioral Health Clinicians (BHC, LICSW) are an integral part of the Collaborative Care Model to integrate behavioral health into primary care. Primary care clinicians are reluctant to prescribe buprenorphine without systems in place, especially behavioral support.
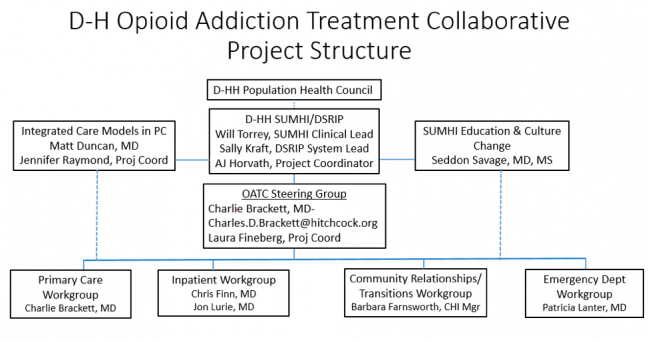
Project structure
Image