
The page contains the following sections:
When is surgical repair of a heart rhythm disturbance advisable?
How is repair of a heart rhythm disturbance accomplished?
What are the risks and benefits of such surgery?
What is involved in a typical recovery?
When is surgical repair of a heart rhythm disturbance advisable?
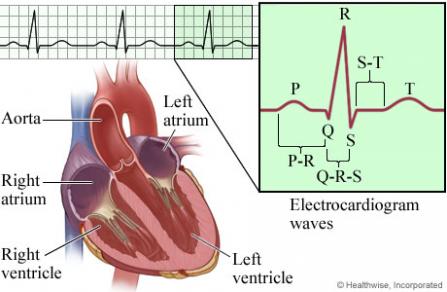
Atrial fibrillation (often referred to as AFib or AF) is the most common kind of arrhythmia, or disturbance of the heart's rhythm. Arrhythmias are caused by a malfunction of your heart's electrical system; in the case of AFib, your heart beats with an irregular rhythm. As a result, not enough oxygen-rich blood may be available to supply your body's needs. This can eventually lead to chest pain, heart failure or the development of blood clots that could result in a stroke (about 15% of strokes occur in people with AFib).
If you are diagnosed with AFib, your surgeon will evaluate the specifics of your situation and help you weigh the risks of cardiac surgery against the risks of continuing to manage the disorder with medication, other nonsurgical treatments or implantation of a pacemaker. Often, if your symptoms are not severe, they can be managed with lifestyle changes and/or medication. Typically, the correction of AFib is performed at the same time as another cardiac procedure—usually, the repair of a defective aortic or mitral valve. Occasionally, however, AFib causes such incapacitating symptoms that cardiac surgery to address the rhythm disturbance is undertaken as a stand-alone procedure.
Should you and your surgeon decide the time is right for surgery, keep in mind that our cardiac surgeons have considerable expertise in all the proven options for the correction of AFib.
How is repair of a heart rhythm disturbance accomplished?
There are several ways to restore your heart to a normal rhythm. Your surgeon will consider various factors—such as your age, the overall state of your health, and whether your AFib is chronic or sporadic—in deciding which of these options will work best:
- Cardiac ablation involves the use of either high-frequency radio waves or extreme cold to destroy the damaged portion of your heart's electrical system. The technique that uses radio waves is known as radiofrequency ablation, and the technique that uses cold is known as cryoablation. ("Ablation" comes from Latin words meaning "take away from" or "remove," while "cryo" comes from a Greek word meaning "frost.")
- A maze procedure involves making tiny cuts known as lesions on the surface of your atriums — in a pattern like a little maze, hence the procedure's name; the lesions disrupt the uncoordinated electrical signals that cause AFib.
- A modified maze procedure, known as the Cox-Maze IV procedure, involves the use of a combination of techniques. Some lesions are created using the traditional maze process and others are created using either radiofrequency waves or cryo-energy (cold). This allows the procedure to be completed much more efficiently.
All of these procedures can be performed via open-heart surgery, minimally invasive surgery or endovascular surgery. When they're done at the same time as another procedure, as is usually the case, the requirements of that operation typically determine which of these surgical approaches is most appropriate:
- Open-heart surgery to correct a heart rhythm disturbance involves making an 8- to 10-inch incision over the middle of the sternum, or breastbone, then dividing the sternum to allow access to the heart. In some cases a less invasive option, involving a slightly smaller sternal incision, is possible. Then the chosen procedure is performed through the incision.
It will be necessary to stop your heart from beating during the procedure, so the operation can be performed on a motionless and bloodless field; while your heart is stopped, a device known as a heart-lung bypass machine will take over your heart's function and maintain your circulation. Very occasionally, during complex operations also involving the aorta, you may be put into a state known as hypothermic circulatory arrest; this involves lowering your body temperature to significantly slow your body's cellular activity, permitting your blood flow to be temporarily stopped. (The term "hypothermic" comes from Greek words meaning "low heat," while "circulatory arrest" means your circulation is arrested, or stopped.) In other cases, a technique known as axillary cannulation (or the insertion of a drainage tube, known as a cannula, in an artery in your armpit, or axilla) can allow aortic replacement to be performed without hypothermic circulatory arrest; this advance may reduce the incidence of postoperative strokes and neurological deficits.
- Minimally invasive surgery involves making one or two smaller incisions (typically 2 to 4 inches) in the side of your chest, between your ribs. Then the procedure is performed by inserting a tiny camera and long, thin surgical instruments through your tissues to your heart. Minimally invasive surgery also requires the use of a heart-lung bypass machine. In addition, it may require a period of hypothermic circulatory arrest. In circumstances when it is appropriate, this approach avoids the need to split the sternum and open the entire chest, so recovery may be faster.
- Endovascular surgery, another type of minimally invasive surgery, involves making a couple of tiny incisions (often just 1 to 2 inches) in blood vessels in your groin; inserting long, thin tubes known as a catheters through the vessels to your heart; and then using X-ray guidance and long, thin instruments threaded through the catheters to perform the procedure. (The term "endovascular" comes from Greek and Latin words meaning "within a vessel.") There is also a specific form of endovascular surgery called transcatheter aortic valve replacement (TAVR).
In circumstances when it is appropriate, endovascular surgery can sometimes be done with the patient under local rather than general anesthesia; in addition, it usually does not require hypothermic circulatory arrest or use of a heart-lung bypass machine. In the relatively rare situation when heart rhythm surgery is done on a stand-alone basis, it can often be done as an endovascular procedure. Since this approach avoids the need to open the chest at all, it usually results in much faster healing.
What are the risks and benefits of such surgery?
It is important to keep in mind that every medical choice involves a trade-off between risks and benefits—whether it is to undergo surgery, take medication, or even just carefully monitor a condition (an option known as "watchful waiting").
In the case of AFib, deciding whether cardiac surgery is advisable involves balancing the risks involved in any heart surgery against the risk of continuing to manage the rhythm disorder (as well as any associated valvular problems) with medication and other nonsurgical treatments.
The risks involved in surgery are typically quite low. Since surgery for AFib is often undertaken at the same time as another surgical procedure, the overall risks are generally the same as for whatever other procedure is being performed. In other words, performing cardiac ablation or a maze procedure does not usually result in any additional risk.
If the correction of the rhythm disturbance is successful—which is the case in between 50% and 70% of patients—the benefits are considerable. Typically, patients can stop taking blood-thinning medication (often referred to by the brand name of Coumadin), their symptoms are relieved, and the progressive damage to their heart is dramatically slowed or halted.
What is involved in a typical recovery?
A typical open-heart procedure takes from 4 to 6 hours, in some cases up to 8 hours; patients are then maintained under general anesthesia for an additional 4 to 6 hours. If their heart is performing well and there is no excess bleeding, they can emerge from anesthesia and have their breathing tube removed. Most patients stay in the ICU until midday of the day after their procedure; if they continue to do well, the drainage tubes in their chest can then be removed and they can be moved to a regular hospital bed later that day.
The typical hospital stay ranges from 4 to 7 days. At that point, the vast majority of patients are able to go home, with support from the visiting nurse service, though about 15% to 30% may need to spend some time in a rehab facility for more extensive rehabilitation. After discharge, patients are advised not to drive for about three weeks and not to lift anything heavier than 5 pounds for about 6 weeks. Beyond that point, they can resume whatever activities they wish to.
Patients tend to be surprised at how easy it is to control their pain. By the second day after their operation, most patients are comfortable without intravenous pain medication, taking only oral painkillers, and the overwhelming majority are discharged home on just Tylenol or Motrin.
In cases when minimally invasive surgery is appropriate, the recovery period may be shorter (much shorter in the case of endovascular surgery).
Page reviewed on: Jun 26, 2018
Page reviewed by: Jock McCullough, MD